

 (Part 1 of 2-parts: )
(Part 1 of 2-parts: )
President Donald Trump, whose administration has been
hamstrung in keeping one of his most significant campaign pledges—to lower the
cost of prescription medicines--, now has apparently decided to take the course
of issuing executive orders to end the tragedy that continues to plague American patients,
namely living in the country with the highest costs prescription medicines of
any industrialized nation in the world and being denied access to vital
medicines.
We have issued news releases and blogs urging that the
President take such action, and move it out of the purview of members of the
U.S. Congress who receive millions of dollars from Pharma in campaign
contributions.
At the same time, we believe the President must accept some of
the burden of the blame for the inaction.
He has appointed a Health and Human Services Secretary, former
Representative Tom Price, who is decidedly pro-Pharma, and who, many believe,
even profited from stock purchases of a Pharma stock that increased
tremendously in value based upon inside knowledge.
Also, the President’s appointee (Scott Gottlieb) as
Commissioner of the Food and Drug Administration (FDA), apparently believes
that the ‘free market’ is the primary tool to lower the costs of over-priced
medicines, and opposes personal importation of safe, affordable brand-name
medicines from licensed, registered pharmacies in Tier One Countries whose
standards of safety and efficacy meet or exceed those of the U.S. He also
opposes negotiation by the government with Pharma, choosing instead to look to
stepped-up introduction of generics as the primary route to lowering the costs
of medicines.
As for Congress, it continues to stumble along with plan after
plan, proposed legislation, including the fatally flawed S. 469, hailed by many
Democrats as the save-all concept to lower prescription drug costs. The bill is based upon an equally flawed
effort of 2003 when it was first introduced. The legislation has already raised
vigorous opposition among groups not only in the U.S. but also in Canada
because it would impose U.S. oversight on Canadian-based operations such as
provincial licensing authorities in Canada, and even Health Canada.
This is more than unfortunate, it is tragic because it
illustrates what can only be considered the politicalization of an important
American healthcare issues, e.g., the beneficial impact upon the health and
well-being of American patients from access to adherence to a regimen of
authentic prescription medicines.
The estimates vary, but the undeniable fact is that millions
of American patients forego such adherence simply because the medicines
themselves are so high-priced that they are unaffordable, making them, in and
of themselves, unavailable.
While we are faced with the spectacle of an ineffective
response from Congress, which continues to offer narrowly defined proposals
ranging from personal importation to transparency to more generics to penalties
for Pharma price gouging , and conducting time-consuming hearings that result
in nothing, while Pharma continues to thumb its collective nose to the American
people and set prices beyond the reach of patients.
At the same time, a score of group and organizations issue
periodic statements, collective letters and develop positions that address the
costs and availability of medicines that costs thousands of dollars, all the
while ignoring the fact that these commendable efforts are not mutually
exclusive from the inclusion as part of recognition of the harmful impact of
lack of access to any medicine, and that an unaffordable maintenance medicine
is just as unavailable to untold numbers of patients as a medicine that costs $120,000 a year.
As an advocate for role for Personal Importation of brand-name
prescription medicines, and as a supporter of a comprehensive approach to
address all elements of the negative impact of Pharma pricing abuses, and the
rapidly evolving record of abuses by huge pharmacy benefit managers, I believe it
is tragic that the discussion about the costs and availability of any medicine
has become so highly segmented.
That is why it is incumbent upon the President to provide leadership by creating policies that will
result in a truly comprehensive solution with personal importation being
recognized as not only a part of his strategies, but as the only offering a
degree of immediate relief to the dilemma of 55 million Americans not being
able to afford their medications.
While many of the challenges of new medicines, value, and
prices will be met in the future, the fact is that personal importation is a
readily, safe available strategy that has already been embraced by millions of
Americans, and has received support from policy-makers at local, state and
Federal levels, even in the face of Pharma opposition and Congressional
inaction!
Why then, has the personal importation of safe, brand-name
medicines from licensed registered pharmacies in Tier One Countries whose standards
of safety and efficacy meet or exceed those of the U.S. not become a part of
the solution when an examination of the facts makes the case for such a
strategy from to allow personal importation of prescription and offer benefits
to the health and well-being of Americans.
For more than a quarter-century, Americans have been victims
of the predatory pricing practices of Pharma.
•
Americans pay the highest prescription prices in
the industrial world
•
This is based upon a national policy of allowing
the industry to ‘charge what the traffic will bear’
•
The Pharmaceutical Industry has created alliances,
influenced governmental policy, colluded with regulatory agencies designed to
ensure prices are affordable, and literally ‘bought’ overwhelmed the U.S.
Congress with the most contributions of any industry segment in the U.S.
•
Result #1—A denial for an estimated 55 million
Americans to be able to exercise their right to the health benefit made
possible from access to a regimen of vital life-line medicines, simply because
they are unaffordable
•
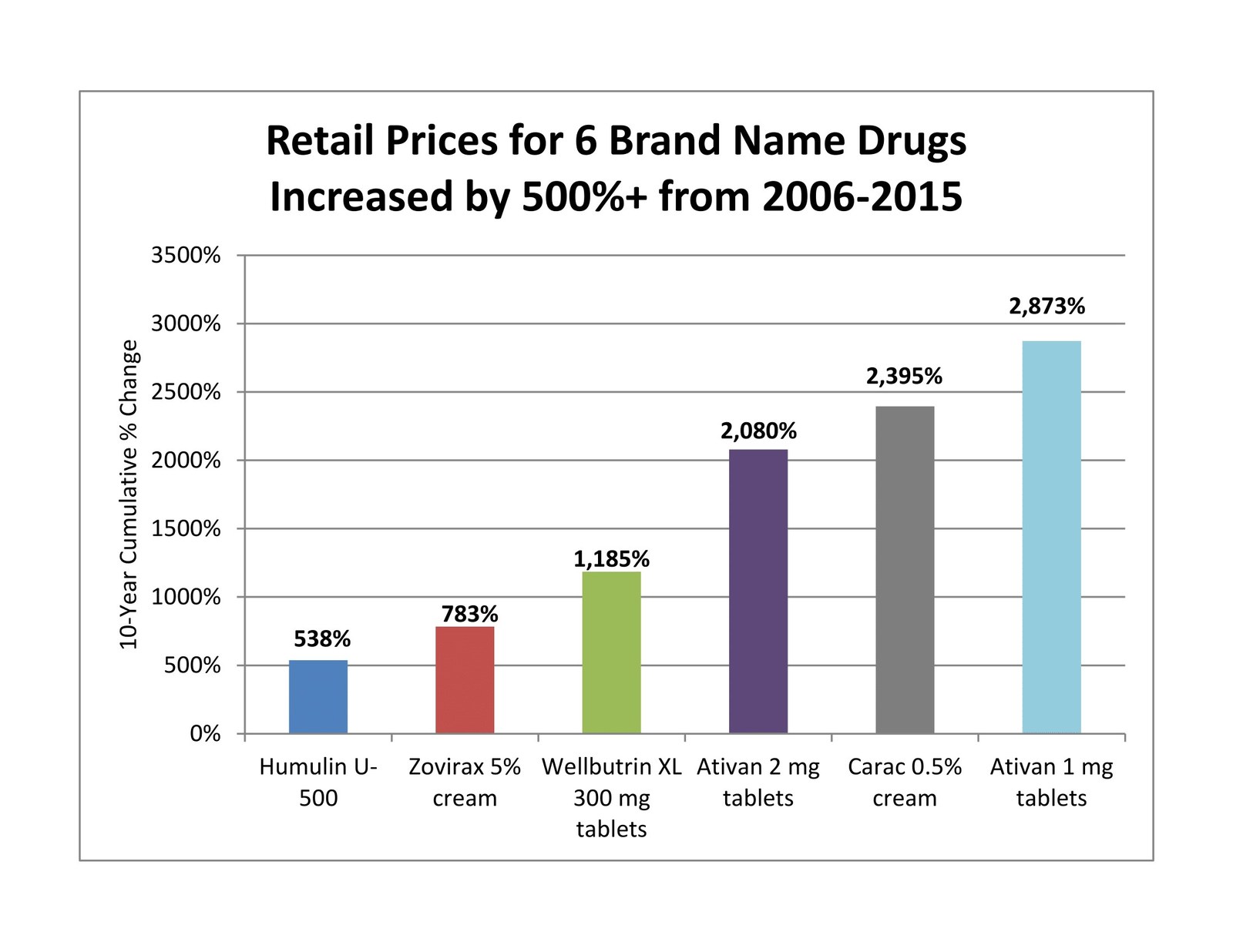
Result # 2—The ‘hoped-for’ answer to the scourge
of unaffordable medicines—generic medicines—have seen price spikes that have
made many of them equally unavailable to American patients.
•
Result # 3—Literally millions of Americans suffer
from diseases—many of them life-threatening—raising the question of a possible
link to the cause-effect impact of unaffordable but vital maintenance medicines
that could have benefitted patients and
deterred the harmful effects of their disease.
•
Result # 4—Pharma raises prices, on specialty
medicines to thousands of dollars for treatments, even though many of the
costly medicines are older, lower-cost medicines, and manufacturers are simply
taking advantage of the illness of Americans.
•
Result # 5—Congress becomes indignant, holds
hearings, witness testify, advocacy groups coalesce to ‘address’ price
challenges, but…prices remain high, Congress continues with more hearings…and
Americans continue to pay the highest prices in the world…WHY?
•
RESULT #6--Because Pharma and its allies in the
House of Representatives and the U.S. Senate who are the beneficiaries of
Pharma’s extensive contributions have controlled the discussion on how to lower
prescription and health care costs while Pharma continues to rake in obscene
profits, and American patients continue to be denied their medicines.
It is time for a change!
American patients can’t wait any longer!










{kind=link}